
About Thyroid Tumor: Core Research Knowledge Overview
Thyroid tumors cover a wide spectrum of pathological phenotypes, ranging from inert benign nodules to highly aggressive malignant lesions. Research priorities not only include systematic pathological classification, but also exploring how gene variation, tumor clonal evolution and metabolic reprogramming affect disease progression. This paper summarizes core biological features of thyroid tumors, focusing on progression mechanisms, metabolic traits and promising targeted drug candidates.
1
Basic Overview of Thyroid Tumors
Thyroid lesions are frequently encountered in endocrinology clinics, with highly diversified biological behaviors. Some lesions stay stable for years without obvious deterioration, while others continuously evolve accompanied by molecular and pathological changes. Clarifying tumor origin, pathological traits and research significance lays a solid foundation for translational medical exploration.
1.1 Definition and Origin of Thyroid Tumors
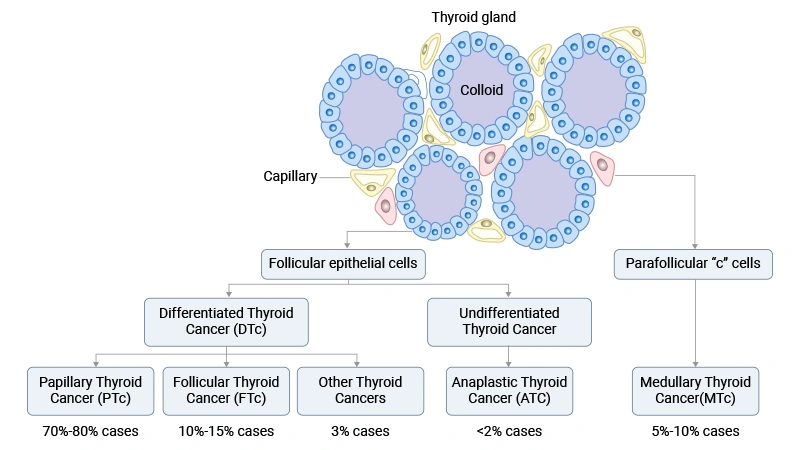
Most thyroid tumors derive from follicular cells responsible for thyroid hormone synthesis, and a small portion originate from parafollicular C cells that secrete calcitonin. Follicular cell-derived lesions contain benign adenomas and differentiated malignant tumors such as papillary carcinoma and follicular carcinoma. C-cell lesions are mainly medullary thyroid carcinoma. Cellular source directly determines biological properties and subsequent therapeutic schemes.
1.2 Research Value of Thyroid Tumors
Thyroid tumors serve as ideal research models to explore tumor initiation, cell differentiation and malignant progression. They distinctly demonstrate the evolutionary process from well-differentiated benign state to invasive malignant phenotype caused by accumulated molecular abnormalities. Hence thyroid carcinoma becomes a typical research object for studying tumor heterogeneity and precise oncology theories.
1.1 Definition and Origin of Thyroid Tumors
Most thyroid tumors derive from follicular cells responsible for thyroid hormone synthesis, and a small portion originate from parafollicular C cells that secrete calcitonin. Follicular cell-derived lesions contain benign adenomas and differentiated malignant tumors such as papillary carcinoma and follicular carcinoma. C-cell lesions are mainly medullary thyroid carcinoma. Cellular source directly determines biological properties and subsequent therapeutic schemes.
1.2 Research Value of Thyroid Tumors
Thyroid tumors serve as ideal research models to explore tumor initiation, cell differentiation and malignant progression. They distinctly demonstrate the evolutionary process from well-differentiated benign state to invasive malignant phenotype caused by accumulated molecular abnormalities. Hence thyroid carcinoma becomes a typical research object for studying tumor heterogeneity and precise oncology theories.
2
Main Classification of Thyroid Tumors
The fifth edition of WHO classification standardizes thyroid tumor grouping standards based on cellular origin and clinical risk grade, dividing lesions into benign, low-risk and malignant types. Follicular cell tumors, C-cell tumors and other rare subtypes are classified separately, matching their inherent biological properties and prognostic differences.
2.1 Follicular Cell-Derived Neoplasms
This category accounts for the largest proportion of thyroid lesions and is divided into three risk grades.
- Thyroid follicular nodular disease (TFND): Hyperplastic nodules generated from multinodular goiter, mostly polyclonal reactive proliferation rather than true neoplastic lesions.
- Follicular thyroid adenoma (FTA): Encapsulated localized tumor without capsule or vascular invasion, possessing no metastatic capability.
- Oncocytic adenoma (OA): Composed of mitochondria-rich Hürthle cells with eosinophilic granular cytoplasm, presenting no invasive pathological features.
Benign lesions share similar morphological appearances with low-risk and malignant tumors, bringing difficulties to pathological identification.
2.1.2 Low-Risk Neoplasms
- Non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): Encapsulated tumor with papillary carcinoma nuclear variation and no invasive manifestation.
- Thyroid tumor of uncertain malignant potential (TT-UMP): Lesion with ambiguous capsule and vascular invasion, lacking sufficient evidence for malignant diagnosis.
- Hyalinizing trabecular tumor (HTT): Rare trabecular lesion with hyaline stroma and papillary-like nuclear characteristics, categorized as low-risk tumor.
2.1.3 Malignant Follicular Cell Tumors
- Papillary thyroid carcinoma (PTC): Dominant clinical subtype occupying 70–80% cases, defined by unique nuclear morphology and frequently accompanied by BRAF and RET pathway mutations.
- Follicular thyroid carcinoma (FTC): Accounts for less than 15% cases, closely correlated with RAS mutation and PAX8-PPARG fusion gene, diagnosed based on invasive capsule and vascular tissue.
- Oncocytic carcinoma (OCA): Malignant Hürthle cell tumor with definite invasive ability.
2.2 C-Cell Derived Thyroid Carcinoma
Medullary thyroid carcinoma (MTC) originates from parafollicular C cells, taking up about 3% of all thyroid tumors. It occurs sporadically or hereditarily due to germline RET gene mutation, and calcitonin can be used as specific diagnostic biomarker. The latest WHO standard further divides MTC into low-grade and high-grade subtypes.
2.3 Mixed Medullary and Follicular Cell Carcinoma
Rare composite tumor containing both medullary and follicular tumor components, capable of expressing calcitonin and thyroglobulin simultaneously, recognized as an independent pathological subtype.
2.4 Salivary Gland Type, Thymic and Other Rare Thyroid Tumors
- Salivary Gland Type Malignant Tumors:Thyroid mucoepidermoid carcinoma, salivary gland-type secretory carcinoma.
- Thyroid Tumors with Unclear Histogenesis:Sclerosing mucoepidermoid carcinoma with eosinophilia, cribriform-morular thyroid carcinoma.
- Thymic and Thymus-Like Tumors: Thymoma, spindle epithelial tumor with thymus-like elements, intrinsic thyroid thymic carcinoma.
- Embryonal Thyroid Neoplasms: Typified by thyroblastoma, featuring primitive tissue structure and specific molecular variation characteristics.
2.1 Follicular Cell-Derived Neoplasms
This category accounts for the largest proportion of thyroid lesions and is divided into three risk grades.
- Thyroid follicular nodular disease (TFND): Hyperplastic nodules generated from multinodular goiter, mostly polyclonal reactive proliferation rather than true neoplastic lesions.
- Follicular thyroid adenoma (FTA): Encapsulated localized tumor without capsule or vascular invasion, possessing no metastatic capability.
- Oncocytic adenoma (OA): Composed of mitochondria-rich Hürthle cells with eosinophilic granular cytoplasm, presenting no invasive pathological features.
Benign lesions share similar morphological appearances with low-risk and malignant tumors, bringing difficulties to pathological identification.
2.1.2 Low-Risk Neoplasms
- Non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP): Encapsulated tumor with papillary carcinoma nuclear variation and no invasive manifestation.
- Thyroid tumor of uncertain malignant potential (TT-UMP): Lesion with ambiguous capsule and vascular invasion, lacking sufficient evidence for malignant diagnosis.
- Hyalinizing trabecular tumor (HTT): Rare trabecular lesion with hyaline stroma and papillary-like nuclear characteristics, categorized as low-risk tumor.
2.1.3 Malignant Follicular Cell Tumors
- Papillary thyroid carcinoma (PTC): Dominant clinical subtype occupying 70–80% cases, defined by unique nuclear morphology and frequently accompanied by BRAF and RET pathway mutations.
- Follicular thyroid carcinoma (FTC): Accounts for less than 15% cases, closely correlated with RAS mutation and PAX8-PPARG fusion gene, diagnosed based on invasive capsule and vascular tissue.
- Oncocytic carcinoma (OCA): Malignant Hürthle cell tumor with definite invasive ability.
- Differentiated high-grade thyroid carcinoma (DHGTC) & Poorly differentiated thyroid carcinoma (PDTC): Intermediate malignant grade between differentiated and anaplastic carcinoma, characterized by active cell division and tissue necrosis.
- Anaplastic thyroid carcinoma (ATC): Highly malignant lethal subtype less than 2% incidence, marked by cellular polymorphism, rapid proliferation and extensive necrotic area.2.2 C-Cell Derived Thyroid Carcinoma
Medullary thyroid carcinoma (MTC) originates from parafollicular C cells, taking up about 3% of all thyroid tumors. It occurs sporadically or hereditarily due to germline RET gene mutation, and calcitonin can be used as specific diagnostic biomarker. The latest WHO standard further divides MTC into low-grade and high-grade subtypes.
2.3 Mixed Medullary and Follicular Cell Carcinoma
Rare composite tumor containing both medullary and follicular tumor components, capable of expressing calcitonin and thyroglobulin simultaneously, recognized as an independent pathological subtype.
2.4 Salivary Gland Type, Thymic and Other Rare Thyroid Tumors
- Salivary Gland Type Malignant Tumors:Thyroid mucoepidermoid carcinoma, salivary gland-type secretory carcinoma.
- Thyroid Tumors with Unclear Histogenesis:Sclerosing mucoepidermoid carcinoma with eosinophilia, cribriform-morular thyroid carcinoma.
- Thymic and Thymus-Like Tumors: Thymoma, spindle epithelial tumor with thymus-like elements, intrinsic thyroid thymic carcinoma.
- Embryonal Thyroid Neoplasms: Typified by thyroblastoma, featuring primitive tissue structure and specific molecular variation characteristics.
3
Pathogenic Mechanism of Thyroid Tumor Development
Thyroid malignant transformation is a progressive multi-stage process jointly driven by oncogene activation, clonal variation, cell dedifferentiation, epigenetic modification and tumor microenvironment screening effect.
3.1 Core Genetic Driving Factors
Abnormal MAPK Pathway Activation:Most follicular-origin thyroid cancers are triggered by mutated BRAF, RAS and RET/PTC genes, leading to persistent MAPK pathway activation. BRAF V600E and RAS variation promote cell proliferation, enhance survival capacity and alter cell differentiation status.
PI3K-AKT Pathway Regulation: This pathway plays a vital role in tumor malignant progression, especially follicular patterned carcinoma. It maintains cell survival state, adjusts metabolic level and accelerates invasive growth, and often co-activates with MAPK pathway in advanced malignant lesions.
3.2 Clonal Evolution and Genomic Instability
Continuous accumulation of gene mutations causes intratumoral clonal heterogeneity, further inducing tumor invasion, postoperative recurrence and drug tolerance. Combined mutations such as BRAF and TERT variation are commonly detected in advanced tumors.
Inactivation of Tumor Suppressor Genes: Defective TP53 and PTEN gene function breaks normal cell growth restriction, elevates genome instability and accelerates cell dedifferentiation progress.
3.3 Cell Dedifferentiation and Functional Loss
Downregulated Thyroid Specific Gene Expression: Reduced expression of iodine transporter and hormone synthesis related genes weakens tumor cell sensitivity towards radioactive iodine treatment.
Evolution to Highly Aggressive Pathology: Tumors gradually develop into poorly differentiated or anaplastic carcinoma, accompanied by accelerated cell division, expanded necrotic scope and strengthened invasive performance.
3.4 Epigenetic and Transcriptional Alteration
Aberrant DNA methylation inhibits tumor suppressor and differentiation-related gene expression. Oncogenic signals rebuild cell transcription profile, facilitating proliferation and stress-resistant phenotype formation.
3.5 Tumor Microenvironment Impact
Stromal fibroblasts, infiltrating immune cells and hypoxic conditions boost angiogenesis, immune escape and dominant tumor clone selection. Reverse Warburg effect enables stromal cell glycolysis to supply energy substances for tumor proliferation.
3.1 Core Genetic Driving Factors
Abnormal MAPK Pathway Activation:Most follicular-origin thyroid cancers are triggered by mutated BRAF, RAS and RET/PTC genes, leading to persistent MAPK pathway activation. BRAF V600E and RAS variation promote cell proliferation, enhance survival capacity and alter cell differentiation status.
PI3K-AKT Pathway Regulation: This pathway plays a vital role in tumor malignant progression, especially follicular patterned carcinoma. It maintains cell survival state, adjusts metabolic level and accelerates invasive growth, and often co-activates with MAPK pathway in advanced malignant lesions.
3.2 Clonal Evolution and Genomic Instability
Continuous accumulation of gene mutations causes intratumoral clonal heterogeneity, further inducing tumor invasion, postoperative recurrence and drug tolerance. Combined mutations such as BRAF and TERT variation are commonly detected in advanced tumors.
Inactivation of Tumor Suppressor Genes: Defective TP53 and PTEN gene function breaks normal cell growth restriction, elevates genome instability and accelerates cell dedifferentiation progress.
3.3 Cell Dedifferentiation and Functional Loss
Downregulated Thyroid Specific Gene Expression: Reduced expression of iodine transporter and hormone synthesis related genes weakens tumor cell sensitivity towards radioactive iodine treatment.
Evolution to Highly Aggressive Pathology: Tumors gradually develop into poorly differentiated or anaplastic carcinoma, accompanied by accelerated cell division, expanded necrotic scope and strengthened invasive performance.
3.4 Epigenetic and Transcriptional Alteration
Aberrant DNA methylation inhibits tumor suppressor and differentiation-related gene expression. Oncogenic signals rebuild cell transcription profile, facilitating proliferation and stress-resistant phenotype formation.
3.5 Tumor Microenvironment Impact
Stromal fibroblasts, infiltrating immune cells and hypoxic conditions boost angiogenesis, immune escape and dominant tumor clone selection. Reverse Warburg effect enables stromal cell glycolysis to supply energy substances for tumor proliferation.
4
Metabolic Traits of Thyroid Tumor Tissue
Thyroid cancer cells generally undergo metabolic reprogramming, mainly presenting enhanced glycolysis intensity, disordered lipid synthesis and abnormal amino acid utilization mode.
4.1 Overall Metabolic Remodeling
- Elevated Glucose Absorption Capacity: Upregulated GLUT1 transporter and key glycolytic enzyme expression improve glucose uptake efficiency, and advanced tumors show strong FDG-PET imaging signals.
- Dominant Glycolytic Metabolism: Typical Warburg effect exists in tumor cells. Aerobic glycolysis provides raw materials and energy required for biological synthesis and rapid cell proliferation.
4.2 Lipid and Amino Acid Metabolic Characteristics
- Endogenous Lipid Synthesis: Enhanced de novo lipogenesis offers components for cell membrane construction and signal transduction. Metabolic patterns vary obviously among different tumor subtypes.
- Amino Acid Utilization Rules: Glutamine metabolism and one-carbon metabolism maintain intracellular synthetic reaction and redox balance stability.
4.3 Metabolic Interaction Within Tumor Microenvironment
Cancer-associated fibroblasts secrete intermediate metabolites to sustain tumor growth. Hypoxic surroundings induce flexible metabolic adaptation of malignant cells.
4.4 Metabolic Differences Among Tumor Subtypes
- Papillary thyroid carcinoma: Glycolysis activity positively correlates with MAPK pathway activation level.
- Follicular carcinoma and advanced malignant tumors: Glutamine and lipid metabolism strengthen along with cell dedifferentiation.
Metabolic regulatory proteins including GLUT1, HK2 and SLC7A5 have become promising novel therapeutic targets.
4.1 Overall Metabolic Remodeling
- Elevated Glucose Absorption Capacity: Upregulated GLUT1 transporter and key glycolytic enzyme expression improve glucose uptake efficiency, and advanced tumors show strong FDG-PET imaging signals.
- Dominant Glycolytic Metabolism: Typical Warburg effect exists in tumor cells. Aerobic glycolysis provides raw materials and energy required for biological synthesis and rapid cell proliferation.
4.2 Lipid and Amino Acid Metabolic Characteristics
- Endogenous Lipid Synthesis: Enhanced de novo lipogenesis offers components for cell membrane construction and signal transduction. Metabolic patterns vary obviously among different tumor subtypes.
- Amino Acid Utilization Rules: Glutamine metabolism and one-carbon metabolism maintain intracellular synthetic reaction and redox balance stability.
4.3 Metabolic Interaction Within Tumor Microenvironment
Cancer-associated fibroblasts secrete intermediate metabolites to sustain tumor growth. Hypoxic surroundings induce flexible metabolic adaptation of malignant cells.
4.4 Metabolic Differences Among Tumor Subtypes
- Papillary thyroid carcinoma: Glycolysis activity positively correlates with MAPK pathway activation level.
- Follicular carcinoma and advanced malignant tumors: Glutamine and lipid metabolism strengthen along with cell dedifferentiation.
Metabolic regulatory proteins including GLUT1, HK2 and SLC7A5 have become promising novel therapeutic targets.
5
Targeted Drugs and Latest Research Progress
5.1 RET Targeted Therapeutic Drugs
Selective RET inhibitors selpercatinib and pralsetinib exert satisfactory treatment effects on RET fusion mutated papillary carcinoma and medullary thyroid carcinoma.
5.2 BRAF and MEK Combined Inhibitors
Joint administration of dabrafenib and trametinib is applied to treat BRAF V600E mutated anaplastic thyroid carcinoma, while acquired drug resistance still remains a tough clinical obstacle.
5.3 Cell Redifferentiation Treatment Strategy
Blocking MAPK pathway activity can recover radioactive iodine sensitivity of refractory thyroid tumor cells and improve subsequent therapeutic outcomes.
5.4 Novel Metabolic Target Exploration
Amino acid transporter SLC7A5 and one-carbon metabolic enzyme SHMT2 are core research directions for new anti-tumor drug development.
Selective RET inhibitors selpercatinib and pralsetinib exert satisfactory treatment effects on RET fusion mutated papillary carcinoma and medullary thyroid carcinoma.
5.2 BRAF and MEK Combined Inhibitors
Joint administration of dabrafenib and trametinib is applied to treat BRAF V600E mutated anaplastic thyroid carcinoma, while acquired drug resistance still remains a tough clinical obstacle.
5.3 Cell Redifferentiation Treatment Strategy
Blocking MAPK pathway activity can recover radioactive iodine sensitivity of refractory thyroid tumor cells and improve subsequent therapeutic outcomes.
5.4 Novel Metabolic Target Exploration
Amino acid transporter SLC7A5 and one-carbon metabolic enzyme SHMT2 are core research directions for new anti-tumor drug development.
Conclusion
Thyroid tumors display heterogeneous biological features determined by cellular origin, driving gene mutation, clonal evolution and metabolic remodeling. Modern research integrates pathological diagnosis, molecular mechanism exploration, metabolic regulation and targeted medication application, steadily promoting the development of precise thyroid tumor treatment system.